
The CDC Data Project
Destroying America’s Public Health Infrastructure: How the RIFs, OMB’s Proposed Budget, and the HHS Reorganization are Gutting CDC
This independent, non-governmental report and accompanying materials summarize entirely publicly available federal agency and budget data. It was developed independently of any federal agency.
Last Updated: 07/2025
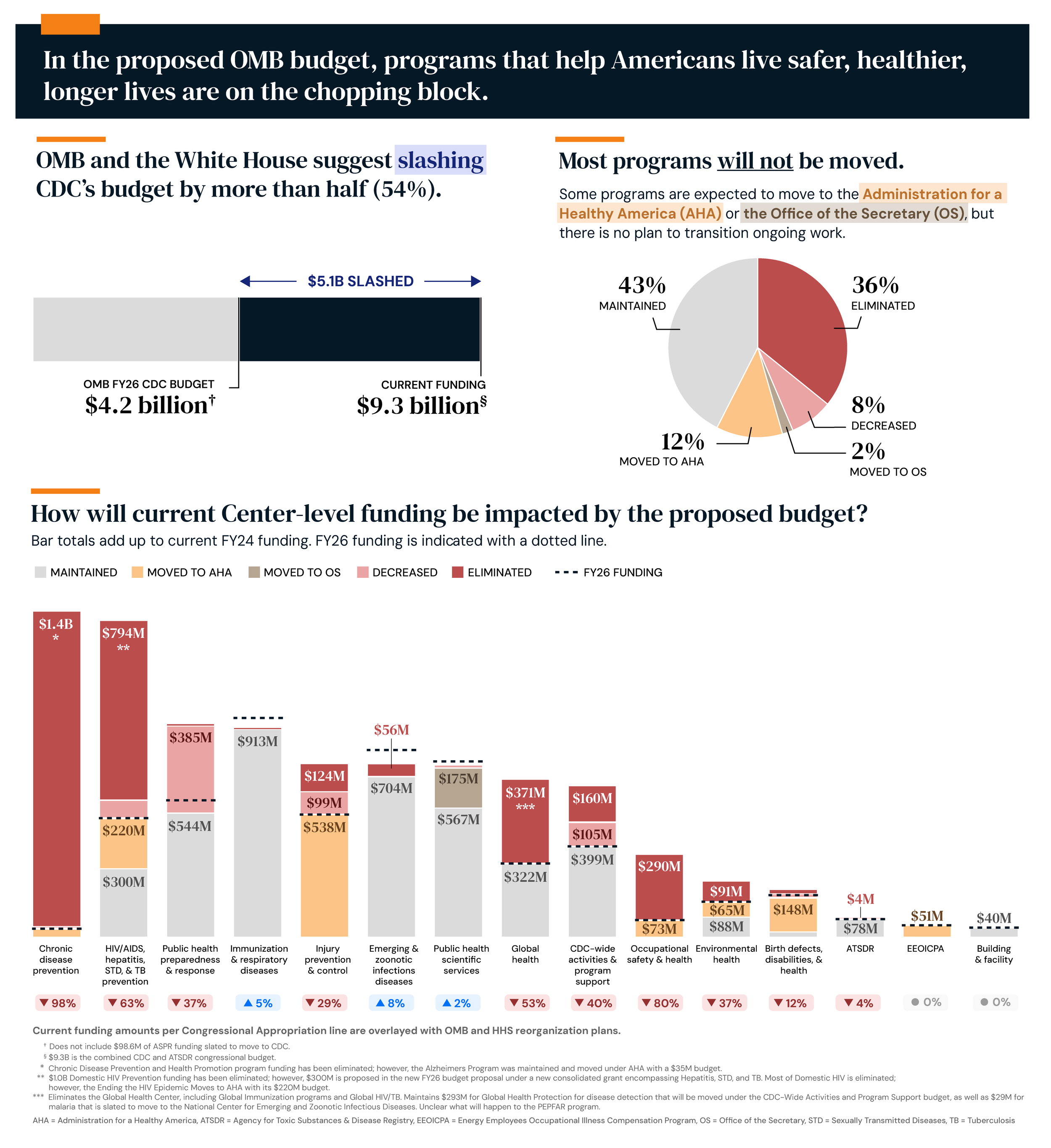
Figure 1. OMB’s Budget Proposal and HHS Re-organization.
RIFs, OMB Proposed Budget, and HHS Reorganization
OMB and the White House Suggest Slashing CDC’s Budget by More than Half (~$5 billion)
The proposed budget represents an unprecedented assault on America's health security, slashing up to 54% of the funding deemed essential by Congress for CDC operations. Figure 1 displays the Centers for Disease Control and Prevention (CDC) current program funding overlaid with the Office of Management and Budget (OMB) and Health and Human Services (HHS) plans to move programs to the Administration for Health America (AHA), the HHS Office of the Secretary (OS), or eliminate entire programs, including the National Center for Chronic Disease & Health Promotion.
Programs that track and combat America's leading killers (heart disease, cancer, diabetes) and others (obesity, maternal mortality, smoking) face elimination despite Make America Healthy Again (MAHA) stated health priorities. The very programs that Secretary Kennedy claims to champion are slated for elimination. If these plans are carried out, this work will collapse, and there will be no way to assess the impact of any MAHA work (Appendix 1, Surveillance Systems).
Very few existing programs are transitioning to the new AHA agency. Despite claims by OMB, CDC leadership, many of whom were RIF’d in April, were not engaged in reorganization or transition planning. No transition plan exists for dedicated staff or their decades of life-saving work. These aren't inefficiencies being trimmed or duplicative programs; these are proven, essential programs being destroyed wholesale.
This isn't about efficiency. Dismantling essential systems and starting from scratch wastes resources, destroys institutional knowledge, and creates dangerous gaps in protection. The most efficient approach would be strengthening existing programs that already work, not obliterating them to build costly, untested replacements.
Critically important public health investments are being unnecessarily and wastefully ignored, upending more than a century of shared values & understanding of public health as a bipartisan public good. The United States has built the world's gold standard in public health innovation, earning global leadership through HHS programs that are both effective and cost-efficient. Our international reputation as pioneers in life-saving health programs – painstakingly built over generations – now faces obliteration.
Prevention is the CDC’s strength. By preventing and reducing chronic diseases, the CDC saves lives, cuts healthcare costs, and sustains a healthy economy.
Public health cuts now mean higher healthcare costs later. In the U.S., diseases like heart disease, cancer, and diabetes combined account for over $1.3 trillion annually in healthcare spending and lost productivity. However, CDC prevention programs have proven extraordinary returns; for example, The Million Hearts® initiative prevented an estimated 135,000 heart attacks, strokes, and other cardiovascular conditions/cardiac events from 2012-2016, averting $5.6 billion in medical costs.
We also know that investing in prevention upfront saves us money in the long term. We save $60 for every $1 spent on flu vaccines for seniors, and yet OMB’s proposed cuts target CDC’s wide range of prevention programs. Their cuts guarantee more outbreaks, ER visits, and higher health costs for taxpayers down the road. American taxpayers will ultimately pay the highest cost.
Impact of Grant Investments on States
The CDC invests 80% of its annual domestic budget in states, tribes, and communities, not D.C. bureaucrats. Eliminating this support will impact every person in the country. In 2023 alone, $4.7 billion in grants supported health departments, hospitals, universities, and nonprofits across the country. Cuts to these investments harm states and local communities far more than CDC workers. On average, nearly 50% of every state’s public health budget comes from HHS. In many states, almost all federal funds are from CDC. Now, over half of that support that directly invests in states’ programs, salaries, training, data collection and use, and innovation is at risk. State and local health departments are forced to consider scaling back public health functions, staffing, and programs they know will weaken their ability to keep their residents healthy and safe, identify and prevent diseases, and respond to emergencies.

Figure 2. Contract and Emergency Investments Already Cut.
🔻An estimated 51% ($7.7 billion) of annual funding is at risk from the RIF, OMB, or part of the March 24, 2025, supplementary funding cut Source: fundingprofiles.cdc.gov, crowdsourced RIF list, OMB budget proposal
🔻 Without any input from Congress, already appropriated funds are being quietly canceled and cut, including $2.9 billion in CDC contracts and $11.4 billion in emergency supplemental public health funding.
Per Capita Loss of Grant Investments in US States
States and Local Communities Stand to Lose the Most: Loss of State Funding Resulting from OMB Budget, HHS Reorganization, and Supplemental Funding Cuts

Figure 3. Annual Loss of CDC Grant Funding resulting from Proposed Eliminations or Reductions in programs, and Supplemental Funding Already Terminated, Per Capita and Total Funding.
Per Capita, rural, Midwest, and Southern states were hardest hit, including Wyoming, North Dakota, South Dakota, Louisiana, and Alaska. State and local health departments have been slashing staff as a result of these cuts.
CDC funding ensures local experts in state and local health departments have the skills, tools, and relationships they need to detect and lead responses to outbreaks and disasters reliably. When CDC funds and programs get cut, local communities and experts lose their backup.
Our frontline health defenses have been quietly gutted through backdoor cuts, bypassing Congress and public debate. This unaccountable action eliminates critical funds, primarily from the Public Health Social Services Emergency Response Fund (PHSSEF) and other COVID-19-related allocations like the American Rescue Plan and CARES Act. This endangers our preparedness and demands immediate attention.
Destroyed CDC Centers and Divisions
Cuts made thus far have targeted and destroyed CDC Centers and Divisions housing decades of data and expertise
Taken together, these cuts are a coordinated hit job that undermines Secretary Kennedy’s leadership, dooms the MAHA agenda, eliminates America’s ability to track, monitor, understand, and fight urgent health threats, and will—even more than it already has—cripple America’s frontline health defenses.
National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP)
Destroying CDC's Work to Fight America’s Most Problematic Health Threats: Cancers, Obesity, Diabetes, Heart Disease, and Maternal Deaths
Current budget proposals suggest eliminating the very CDC Center that carries out all MAHA-related work, the NCCDPHP, undermining the Secretary’s ability to carry out this work.
These programs are already MAHA-aligned, highly functioning, welcomed, and respected by state and local partners, and are essential to achieving MAHA goals.
These programs are the most cost-effective way for communities to Make America Healthy Again. By proposing to shut down this Center, OMB and the White House are setting Secretary Kennedy up to fail.
This Center’s work protects Americans from the top causes of death—heart disease, diabetes, obesity, and cancer.
These programs are necessary, frugal, and effective. CDC funds empower state and local partners to generate $60 in additional non-federal funds for every dollar CDC invests. This is an ROI no private company can match.
Currently, nearly 90% of the $4.5 trillion spent every year on healthcare costs is tied to chronic disease and mental health conditions. Without the CDC programs that help all Americans combat these conditions, that total will explode, and all Americans will pay that price.
Just as millions of veterans, mothers, and seniors face increasing health threats, the RIF came in and eliminated CDC’s leading effective work on healthy aging, the Prevention Research Centers, surveillance, reproductive health, oral health, and tobacco and vaping.
Cross-Center Public Health Preparedness and Response
Slashing Local Disaster and Disease Preparedness Investments—Abandoning States and Leaving Them Defenseless
CDC was established to ensure Americans would be protected against urgent and unpredictable public health threats. The obligations that accompany this responsibility are more dire now than ever before. In every state, CDC is the primary investor in state and local community public health preparedness activities. Abandoning this post should never be an option.
OMB has already stolen $11.4 billion in Congressionally appropriated CDC preparedness investments directly from states. Now, OMB and the White House want to leave states and local governments to go it alone and scramble and beg their way through their next hurricane, fentanyl outbreak, or foreign biothreat while all these threats are rising.
OMB and White House plans to substantially reduce state and local preparedness and response capacity for effective planning, coordination, capacity, and infrastructure building invite malicious foreign actors to seek out resulting vulnerabilities in frontline readiness for pandemics, hurricanes, and bioterror threats, introducing unnecessary and potentially catastrophic threats to all types of communities.
We wouldn’t cut the military when threats are rising. We shouldn’t cut the CDC when biosecurity threats—from fentanyl to foreign lab leaks—are growing.
National Center for Environmental Health (NCEH) & National Institute for Occupational Safety and Health (NIOSH)
Cutting Environmental Health and Worker Safety, Including Lead Poisoning Prevention and Miner Safety and Health.
OMB killed CDC’s flagship programs that are unanimously recognized as the promises we make to the children we love and the miners who literally make it possible for the rest of us to keep the lights on.
The miners who do the work we all need to extract valuable minerals and ores from our land deserve to do so without suffering from the deadly lung infections that killed their fathers and grandfathers. By killing CDC’s miner health and safety programs, we doom them to suffer those same fates. Although some have been brought back, mining work in Spokane and the Western States Division is still halted.
Our disregard for the need for reliable and non-commercially biased standards for protective gear for frontline workers and emergency responders puts millions of U.S. workers—nurses, firefighters, farmers, oil and gas crews, warehouse and factory workers—at fatal and unnecessary risk.
Reducing these efforts risks increased exposure to environmental hazards, particularly in children and workers in hazardous industries.
The RIF has already eliminated work including asthma and air quality, lead poisoning, waterborne diseases, food safety, environmental policy research, the black lung program, and personal protective equipment. Some of these staff have been reinstated; however, several programs, including asthma, were already impacted during the RIF and have since been eliminated in the FY26 budget, leaving the long-term outlook of these programs unclear.
For over 50 years and as a statutory entity, NIOSH has been preventing work-related injuries, illnesses, and deaths, and improving the health and well-being of workers across different industries, from agriculture to mining, healthcare workers and retail workers, oil and gas extraction to the food service industry.
NPPTL alone supports more than 20 million U.S. workers who rely on Personal Protective Equipment (PPE) to keep them safe from on-the-job hazards, including frontline workers and emergency responders.
Global Health Center (GHC) - Division of Global HIV and TB
Staff cuts threaten U.S. health security and a trusted bipartisan success.
With USAID and HRSA’s global HIV roles eliminated or substantially diminished, the CDC Division of Global HIV & TB now leads a large part of PEPFAR implementation. Only 24 of the 146 staff RIF’d have been reinstated, slashing staff supporting global health workforce efforts, maternal and child health, and resource optimization programs to support transition to national ownership. Further cuts undermine a program that has saved 25+ million lives globally, protected the U.S. from HIV and TB threats, delivered a strong return on investment, and earned bipartisan support for over 20 years.
National Center for Birth Defects and Developmental Disabilities (NCBDDD)
Cutting Programs for Children with Disabilities and Genetic Disorders
Entire teams within the National Center for Birth Defects and Developmental Disabilities that worked on blood disorders surveillance and research, and disability and health promotion were RIF’d, decreasing protection for infants, Americans with disabilities, birth defects, and blood disorders like hemophilia, thalassemia, and sickle cell disease.
The now-canceled Congressionally mandated Early Health Detection and Intervention Program was responsible for raising newborn screening to 96%, and following up with appropriate diagnostic screening and early intervention.
Statutorily Mandated Health Programs
Ignoring Congress, Gutting Statutorily Mandated Health Programs
Congress established the $1.2 billion Prevention and Public Health Fund (PPHF) to fight chronic disease and boost local health. OMB is now defunding most of it behind closed doors, even though it's the law. These programs save money and lives.
PPHF supports smart, evidence-based investments to fight chronic disease, reduce smoking, and strengthen local health systems. Focusing on prevention helps cut costly treatments, boost life expectancy, and ensure communities are better prepared for health threats without growing government bureaucracy.
The RIF has already impacted PPHF’s Tobacco prevention & reduction efforts and Childhood Lead Poisoning funding.
The Offices of Minority Health and Women’s Health are Congressionally mandated to exist within CDC to develop and deliver life-saving public health research and programs, yet all their civilian staff have been RIFed, gutting the Offices' capacity to carry out their legally required work. These experts played critical roles in emergency responses and public health planning, ensuring that CDC reached all Americans, including minority communities, women, individuals with disabilities, faith-based organizations, and people across all geographic regions. Dismantling the Offices is stopping major mechanisms for delivering effective and culturally appropriate public health interventions, abandoning hundreds of millions of Americans. (Appendix 2, Statutorily Mandated Programs)
A full list of eliminated programs can be found in Appendix 3, Eliminated Programs.
Loss of CDC Staff
OMB's War on America's Health Defenders
The CDC Reduction in Force (RIF) affected close to 2,700 employees, substantially more than the 2,400 cited by Secretary Kennedy.
Nearly 60% of the RIF'd staff in April were public health experts and other types of scientists — not bureaucrats. They fight obesity, diabetes, heart disease, cancers, and respond to biothreats. Appendix 4, RIFs Dashboard, provides a visual overview of RIF’d staff at CDC. Many of these scientists were also members of surge response teams that support the agency’s preparedness and emergency response efforts.
Many of the RIF’d staff held unique, non-duplicative roles despite Secretary RFK Jr.’s claims. In some cases, their responsibilities have not been eliminated, but are instead being absorbed by remaining staff in other offices or conducted by contractors.
While nearly 20% of FTEs—mostly scientists—were reinstated on June 11, more than a thousand scientists remain impacted by the RIF. The Secretary’s decision to reinstate a subset of staff may have been intended to support his claim that 20% were reinstated due to error. The rationale behind these reinstatement decisions remains unclear, particularly given that some programs with reinstated staff are proposed for elimination or transfer to other agencies (e.g., AHA). This has raised questions about the consistency, thoughtfulness, and transparency of the decision-making process. Some examples below:
Staff were reinstated to the Environmental Health programs, such as the Asthma and Air Quality Branch and the Environmental Public Health Tracking Branch, even though these programs are proposed for elimination in the FY26 proposed budget.
Most staff supporting Domestic HIV programs were reinstated, despite close to 80% of their funding being proposed for elimination in the proposed budget.
Many staff from the Division of Global HIV and TB remain RIF’d, even though their funding is expected to continue through the Department of State.
In some cases, staff supporting programs being moved to AHA, such as those working on Alzheimer’s initiatives, remain RIF’d despite their programs retaining funding in the FY26 budget proposal, further contributing to confusion around the decision-making process.
Staff were RIF’d based on program cuts, not merit or tenure, resulting in the loss of public health experts, including many with decades of experience and strong performance records at the agency.
This wasn’t belt-tightening; it was a direct hit on the people all Americans rely on - the ones who track outbreaks, respond to health emergencies, prevent chronic diseases, and protect communities from emerging threats.
Actions to reduce the federal workforce have already had, and are expected to continue having, a significant impact on the size of the CDC workforce. Collectively, close to 4,000 staff have been lost through probationary terminations, voluntary separations (including deferred resignation and early retirement), and the RIF implemented in early April. An additional 1,200 employees are at risk due to proposed funding eliminations for the programs they support, which could lead to further RIFs.
Based on the programs slated to move to AHA, approximately 1,400 CDC staff may be impacted or transferred to the new agency. However, the FY26 Congressional Justification for AHA suggests that meeting this number of transfers from CDC is unlikely, given that the allocated FTEs must also account for staff transfers from HRSA, SAMHSA, and OASH, agencies whose programs make up the majority of AHA’s proposed budget. However, no transition plans have been discussed or shared.
Sources
This report has been compiled utilizing entirely publicly available federal agency and budget data. The Office of Management and Budget (OMB) released the Presidential Budget request in May 2025, followed by the release of the Health and Human Services (HHS) Fiscal Year 2026 (FY26) Budget in Brief and Congressional Justifications for the Centers for Disease Control and Prevention (CDC) and the Administration for a Healthy America (AHA) in early June 2025. This dashboard was developed to present data on the funding and programmatic changes proposed for the Centers for Disease Control and Prevention (CDC) for Fiscal Year (FY) 2026, which begins on October 1, 2025. It aims to raise awareness and promote transparency using the most current information provided on the scope and type of funding and personnel changes.
Centers for Disease Control and Prevention. (n.d.). Grant funding profiles. Centers for Disease Control and Prevention. https://fundingprofiles.cdc.gov
Presidential Budget request https://www.whitehouse.gov/wp-content/uploads/2025/05/Fiscal-Year-2026-Discretionary-Budget-Request.pdf
Health and Human Services (HHS) Fiscal Year 2026 (FY26) Budget in Brief https://www.hhs.gov/sites/default/files/fy-2026-budget-in-brief.pdf
Congressional Justifications for the Centers for Disease Control and Prevention (CDC) https://www.cdc.gov/budget/documents/fy2026/fy-2026-cdc-cj.pdf and the Administration for a Healthy America (AHA) https://www.hhs.gov/sites/default/files/fy-2026-aha-cj.pdf
Cossaeditor. (2025, April 29). Leaked HHS Passback budget includes NIH reorganization, cuts to health agencies: Consortium of Social Science Associations (COSSA). https://cossa.org/leaked-hhs-passback-budget-includes-nih-reorganization-cuts-to-health-agencies
Josh Michaud, J. K. (2025, April 21). CDC’s funding for state and Local Public Health: How Much and where does it go? KFF. https://www.kff.org/other/issue-brief/cdcs-funding-for-state-and-local-public-health-how-much-and-where-does-it-go
This independent, non-governmental report and accompanying materials summarize entirely publicly available federal agency and budget data. Its development was independent of any federal agency. This document is a work in progress and reflects our current understanding based on the best information available to us at this time. While we’ve made every effort to ensure accuracy, there may be gaps or updates needed as new information emerges. We welcome any feedback, corrections, or suggestions to help improve it.
Appendices
Appendix 1. Surveillance Systems Affected by RIF or OMB Cuts (Not Exhaustive)
Appendix 2. Statutorily Mandated Programs
Appendix 3. CDC Eliminated Programs in the FY26 Budget Proposal
Appendix 4. RIFs Dashboard
Suggested Citation for Entire Report: CDC Data Project (2025). “Destroying America’s Public Health Infrastructure: How the RIFs, OMB’s Proposed Budget, and the HHS Reorganization Are Gutting CDC.” Published Online at cdcdataproject.org. Retrieved [DATE] from https://www.cdcdataproject.org/read-the-report.
Suggested Citation for Report Sections (Example, Please Revise as Appropriate): CDC Data Project (2025). “RIFs, OMB Proposed Budget, and HHS Reorganization.” Published Online at cdcdataproject.org. Retrieved [DATE] from https://www.cdcdataproject.org/read-the-report#report-section-1.
Suggested Citation for Report Subsections (Example, Please Revise as Appropriate): CDC Data Project (2025). “Destroyed CDC Centers and Divisions: National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP).” Published Online at cdcdataproject.org. Retrieved [DATE] from https://www.cdcdataproject.org/read-the-report#report-section-4-1.